
Shoulder
 Guided injection of the subacomial bursaRuptured InfraspinatusHydrodistension injection for frozen shoulderRuptured subscapularis tendonHydrodistension of the right glenohumeral joint for frozen shoulderSternoclavicular joint: OsteoarthritisHydrodistension of the glenohumeral joint for frozen shoulder
Guided injection of the subacomial bursaRuptured InfraspinatusHydrodistension injection for frozen shoulderRuptured subscapularis tendonHydrodistension of the right glenohumeral joint for frozen shoulderSternoclavicular joint: OsteoarthritisHydrodistension of the glenohumeral joint for frozen shoulderAnkle & Foot
Plantaris tendonMorton's NeuromaMedial Ankle FHL Tibial Artery and Tibial NerveInjection of the Tibialis tendon sheathPlantar Fascia: Stress Test46 year old female distance runner. Recently changed to a very low profile unsupportive running shoe during the build up to a Marathon. Within 2 weeks she noted quite severe medial ankle pain and was unable to continue training.
UltrasoundUltrasound demonstrated a marked tenosynovitis with synovial thickening within the tibialis posterior tendon sheath around the posterior aspect of the medial malleolus. The tendon itself demonstrated no evidence of significant tendinopathy or tear. Treatment consisted of analysis of foot position and gait. A pronated foot type being noted. A more supportive running shoe was advised with a relatively rigid mid-sole. Orthotics were supplied for everyday footwear to off-load the tendon. In addition after consenting and under ultrasound guidance the tendon sheath of tibialis posterior was injected with 25mg hydrocortisone and 5mls 1% local anaesthetic. The patient was advised on a slow return to running in 1 week. They were unable to complete the Marathon but within 1 month had increased their running to previous levels.
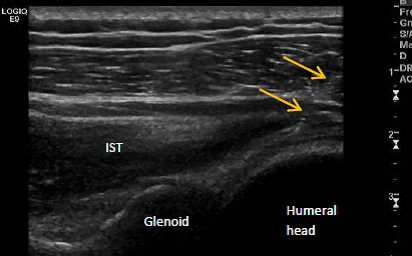
A 76 year old lady was referred from orthopaedics following a fall onto their shoulder 1-month previously. Initially seen in the Emergency Department X-ray had demonstrated no fracture. The patient's main complaint was weakness with normal everyday activity.
UltrasoundUltrasound demonstrated a rupture of the supraspinatus tendon which is not an uncommon finding. However, examination also demonstrated a complete rupture of the tendon of infraspinatus with associated swelling noted in the posterior aspect of the glenohumeral joint extending around the proximal stump of the tendon. A much less commonly noted finding.
A 48 year old male patient with 6 month history of shoulder pain. Onset had been insidious with no initiating trauma. The patient worked as a carpenter and was struggling having been forced to take several occasional days off work. His G referred him to Orthopaedics. An x-ray was unremarkable. A diagnosis of frozen shoulder was made and after little improvement with a course of rehabilitation the patient was referred for an ultrasound guided hydrodistension of the glenohumeral joint.
UltrasoundExamination revealed a clear capsular restriction in range of movement. Lateral rotation - 20 degrees; glenohumeral abduction 30 degrees.
Ultrasound examination was unremarkable.
After consenting the glenohumeral joint was injected using a posterolateral approach with 40mg Depomedrone, 5mls 1% local anaesthetic and 30mls normal saline.
Immediately post-injection range of movement had improved. Lateral rotation - 40 degrees; glenohumeral abduction 70 degrees.
The patient was advised on immediate continuance of their programme of rehabilitation.
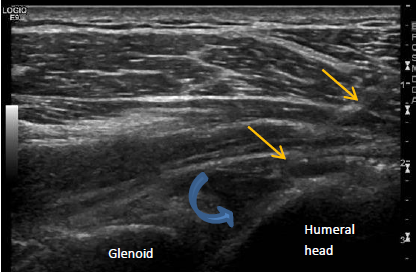
The images demonstrate needle placement into the posterior aspect of the glenohumeral joint. The needle can be seen (yellow arrows) and the saline injected (blue curved arrow).
The patient was a 60 year old keen power lifter who felt a sudden tearing sensation while bench pressing. The US demonstrates a clear complete rupture of the subscapularis tendon.
The patient presented with a 6 month history of right frozen shoulder. This had failed to respond to conservative treatment including exercise and an injection of corticosteroid.
After consenting and using a posterolateral approach the glenohumeral joint was injected with 40mg Depomedrone, 10mls 1% lignocaine and 30mls normal saline.
UltrasoundDuring the injection the capsule maybe seen to stretch and then suddenly release as adhesions are ruptured. The patient noted an improvement in range immediately post injection of some 40 degrees abduction. In this video the needle is just off the left side of the video.
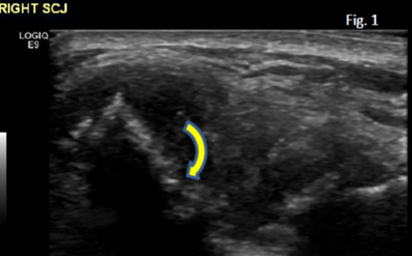
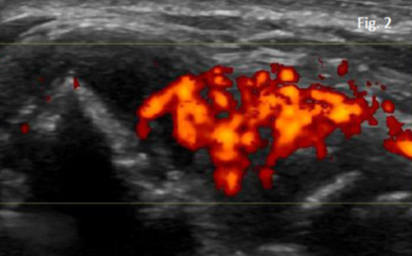
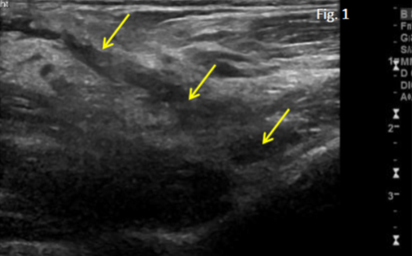
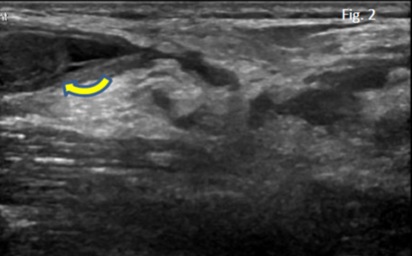
The patient described an insidious onset of right sternoclavicular joint pain over several months duration. Examination demonstrated pain towards end of range shoulder movements in all directions. A prominent and tender right sternoclavicular joint was noted.
UltrasoundUltrasound demonstrates marked cortical irregularity of the right sternoclavicular joint particularly at the proximal clavicle (Fig.1 Curved arrow). In addition there appears to be marked joint hypertrophy which on Power Doppler demonstrated a florid synovitis (Fig. 2).
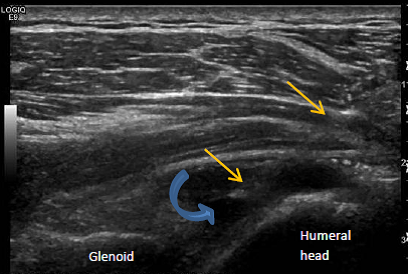
The patient presented with an 8-month history of frozen shoulder. Conservative rehabilitation had failed to date. An injection was undertaken after consenting using a posterolateral approach with 40mg Depomedrone 10mls 1% lignocaine and 30mls of saline. The needle maybe seen to approach the posterior aspect of the glenohumeral joint to sit just below the posterior labrum.
UltrasoundAfter initial injection of the Depomedrone and lignocaine the joint is injected with saline. The posterior capsule maybe seen to stretch away from the posterior humeral head.
40 year old male triathlete with midsubstance Achilles pain of several months duration. Able to run but limited in terms of distance by pain. Stiff Achilles AM. Had been compliant with a programme of eccentrics and stretch. Gait analysis had suggested use of a motion control-like shoe. Pain had persisted and the patient was referred for an Ultrasound.
UltrasoundUltrasound failed to demonstrate any significant tendinopathy or partial tear within the Achilles. However, the patients site of pain correlated with insertion of the tendon of plantaris onto the medial aspect of the Achilles. After consenting and under ultrasound guidance a needle was placed between the plantaris insertion and the Achilles and an injection was carried out using 25mg hydrocortisone and 3mls 1% local anaesthetic. The patient was advised to return to their rehabilitation programme of eccentric loading and stretching after 2 days and then return to running after 2 weeks. At a 1-month review they reported a significant improvement in symptoms and were slowly increasing their running distance.
This transverse image at the level of the metatarsal heads demonstrates a low echo foci between the 3rd and 4th metatarsal heads moving in a plantar direction when the metatarsal heads are squeezed together - A positive Mulder's Click. The image is classic for a Morton's Neuroma
This longitudinal image through the tarsal tunnel at the medial ankle joint demonstrates well the difference in appearance of tendon, nerve and blood vessel. The great toe is being flexed and extended and the deepest structure on the image the tendon of flexor hallucis longus (FHL) can be seen to glide freely in the tunnel. The overlying tibial nerve (N) appears of courser appearance and remains static. The most superficial structure is the posterior tibial artery (A).
46 year old female distance runner. Recently changed to a very low profile unsupportive running shoe during the build up to a Marathon. Within 2 weeks she noted quite severe medial ankle pain and was unable to continue training.
UltrasoundUltrasound demonstrated a marked tenosynovitis with synovial thickening within the tibialis posterior tendon sheath around the posterior aspect of the medial malleolus. The tendon itself demonstrated no evidence of significant tendinopathy or tear.
Treatment consisted of analysis of foot position and gait. A pronated foot type being noted. A more supportive running shoe was advised with a relatively rigid mid-sole. Orthotics were supplied for everyday footwear to off-load the tendon.
In addition after consenting and under ultrasound guidance the tendon sheath of tibialis posterior was injected with 25mg hydrocortisone and 5mls 1% local anaesthetic.
The patient was advised on a slow return to running in 1 week. They were unable to complete the Marathon but within 1 month had increased their running to previous levels.
Longitudinal view of a normal plantar fascia. This video clip demonstrates a stress test of the fascia testing for partial or complete rupture. The fascia in this clip can be seen to be intact.
40 year old climber with triggering of the left index finger. Problems were of insidious onset and had been present for 8 months. 2 blind injections given by the patients GP had been of no benefit.US demonstrated intact tendons of flexor digitorum profundus and superficialis. There was no fluid or synovitis noted within the flexor sheath. Active imaging did however demonstrate some catching of the tendons at the level of the A1 pulley which appeared thickening.
UltrasoundAfter consenting and under ultrasound guidance a needle was introduced deep to the A1 pulley just anterior to the flexor tendons. The needle was used to ensure the tendon was free from the overlying sheath and injection given of relatively high volume to stretch the sheath. In total 12mg hydrocortisone and 3mls of 1% local anaesthetic were injected.
No triggering was present immediately post injection and the patient had returned to full climbing without problems at review 1-month later.
38 year old male. Mixed martial artist. Right thumb twisted while fighting 4 weeks previously. Attended the Emergency Department and advised on rest and ice. XR taken no bony injury.
1 month later pain persisting and attended our Sports Medicine Clinic. Examination revealed tenderness around the ulnar aspect of the right thumb metacarpophalangeal joint with a feeling of increased laxity.
UltrasoundUltrasound demonstrated a rupture of the supraspinatus tendon which is not an uncommon finding. However, examination also demonstrated a complete rupture of the tendon of infraspinatus with associated swelling noted in the posterior aspect of the glenohumeral joint extending around the proximal stump of the tendon. A much less commonly noted finding.
Transverse view of the lower third of the extensor compartment of the forearm demonstrating a normal proximal intersection. The tendons of abductor pollicis longus and extensor pollicis brevis can be seen crossing the tendons of extensor carpi radialis longus and brevis. There is no evidence of pathology.
Transverse view of the dorsal compartments of the wrist at the level of the distal radius. The tendon of extensor pollicis longus can be seen as it leaves the 3rd dorsal compartment to the left of Lister's tubercle and crosses the tendons of extensor carpi radialis logus and brevis in the second dorsal compartment.
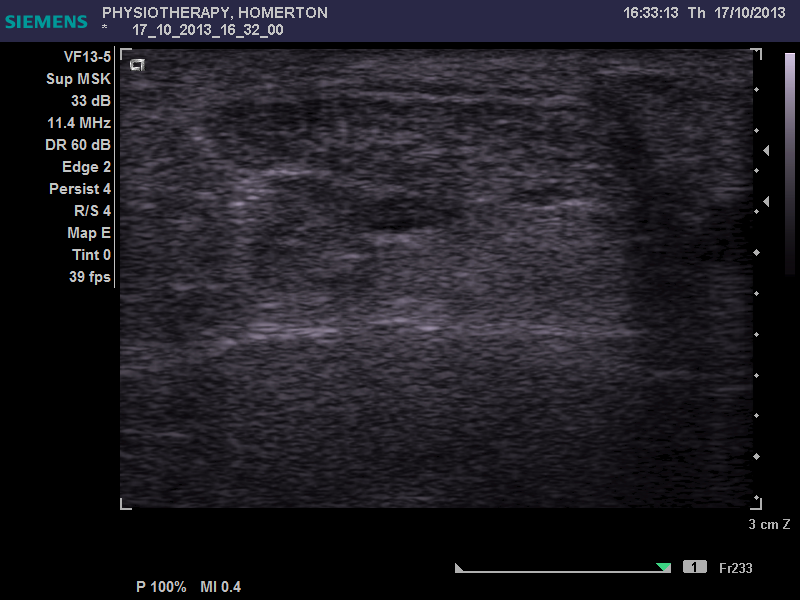
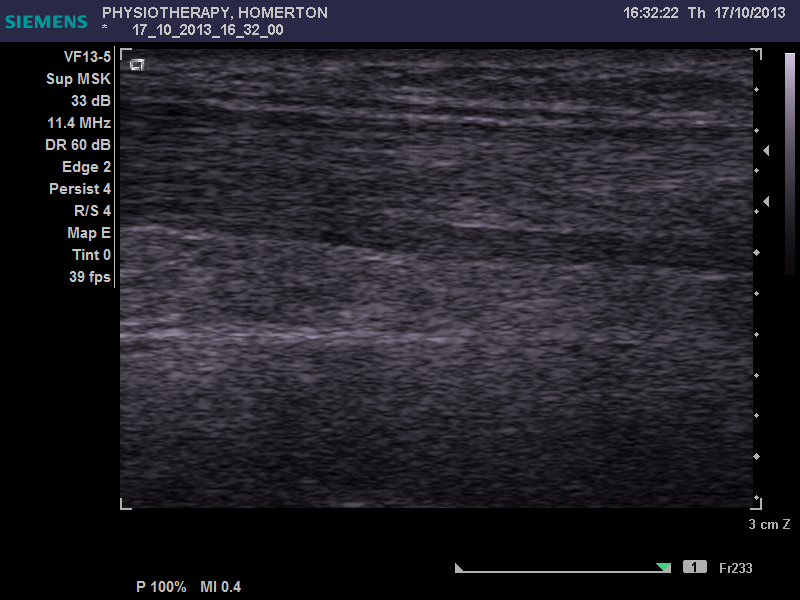
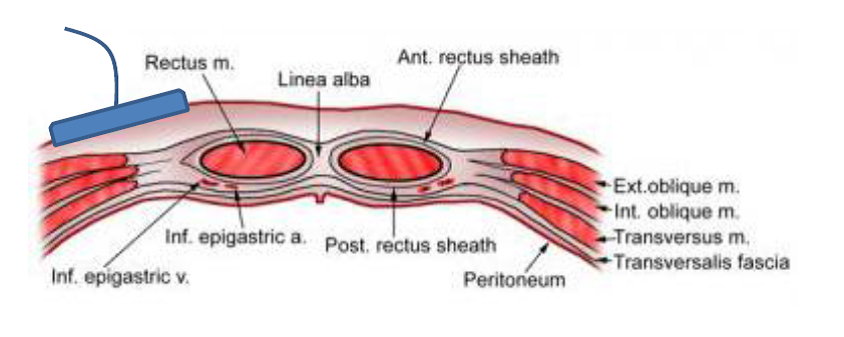
This video is taken with the ultrasound probe over the internal oblique, external oblique and transverse abdominus muscles. (diagram below). The patient had a chronic mechanical back pain with poor activation of the trunk stability muscles. Ultrasound was used to give the patient feedback allowing better activation of the transverse abdominus muscle.
When correctly engaged the transverse abdominus may be seen to contract below the external and internal oblique muscles. When incorrectly engaged all three muscle layers appear to contract equally.
The patient was a 34 year old male and keen sportsman who had been diagnosed as having a femoral acetabular (FAI) impingement of the right hip. An MRI confirmed injury to the anterosuperior labrum. Rather than surgery a conservative approach was taken which included a guided injection.
UltrasoundUltrasound demonstrated no significant cortical irregularity or degenerative change however the anterosuperior labrum appeared irregular and hypertrophied in keeping with FAI.
The injection was given using an anterolateral approach with 40mg Depomedrone and 2mls 1% local anaesthetic.
The patient a 38 year old weight lifter described a sudden onset of right elbow pain following a clean & jerk manueuvere in the gym 3 days previously. Clinically there was a 'reverse-popeye' sign with loss of normal biceps contour suggestive of a rupture of the distal biceps tendon.
UltrasoundUltrasound demonstrated a complete loss of the normal tendon fibrillar pattern in longitudinal view (Fig. 1: yellow arrows). Imaging more proximally demonstrated the retracted stump of the tendon surrounded by swelling and soft tissue oedema (Fig. 2: curved arrow).
transverse view of the suprapatellar region demonstrating an effusion deep to the quadriceps tendon. The needle can clearly be seen moving into the suprapatellar pouch from a lateral direction
Transverse view of the medial patellofemoral joint demonstrating a large bony loose body (note acoustic shadowing).