
Case 8: The Case of the missing Coracoid
A 26 year old male patient was referred with ‘Shoulder impingement +/- injection’. The referral contained no other clinical information. On questioning the patient described surgery for previous shoulder dislocation but could give no other information.
Of interest was the longitudinal scan of the subscapularis tendon and coracoid. Normal scan with associated image is shown below.

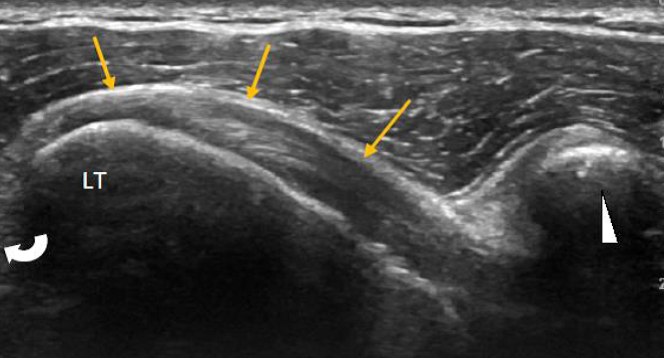
Normal – Longitudinal scan of the subscapularis tendon. The coracoid is shown to the right of the image (white arrowhead). The subscapularis tendon (yellow arrows) maybe seen extending from below the coracoid to insert onto the lesser tuberosity (LT). The curved arrow indicates the relative position of the bicipital groove.
However, when scanning the patient no coracoid was seen (white arrowhead),
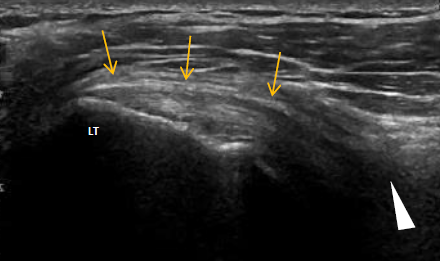
Longitudinal scan of the subscapularis tendon. This is the same view as the previous ‘normal’ image. However, no coracoid maybe seen (white arrowhead).
The patient had undergone a Latarjet proceedure for recurrent anterior dislocation.
The Latarjet operation is a surgical procedure used to treat recurrent anterior shoulder dislocation caused by bone loss or a fracture of the glenoid. The procedure was first described by French surgeon Dr. Michel Latarjet in 1954.
The procedure involves the removal and transfer of a section of the coracoid process and its attached muscles to the front of the glenoid. This acts as a bony block which, combined with the transferred muscles acting as a strut, prevents further dislocation of the joint.
With appropriate patient selection, the Latarjet procedure can be expected to prevent recurrent anterior instability in approximately 94-99% of cases (1,2,3,4,5). Full recovery can take 6 months, however the majority of activities can be resumed after 3 months. The main long term side effect is reduced external rotation range in the shoulder.

References
- Allain, J; Goutallier D; Glorion C (1998). “Long-term results of the Latarjet procedure for the treatment of anterior instability of the shoulder”. J Bone Joint Surg Am. 80(6): 841–52.
- Burkhart, SS; De Beer JF; Barth JR; Cresswell T; Roberts C; Richards DP (2007). “Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss”. Arthroscopy. 23 (10): 1033–41.
- Hovelius, LB; Akermark C; Albrektsson B; Berg E; Körner L; Lundberg B; Wredmark T (1983). “Bristow-Latarjet procedure for recurrent anterior dislocation of the shoulder. A 2-5 year follow-up study on the results of 112 cases”. Acta Orthop Scand. 54 (2): 284–90
- Hovelius, L; Sandström B; Sundgren K; Saebö M (2004). “One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: study I—clinical results”. J Shoulder Elbow Surg. 13 (5): 509–16.
- Walch, G; Boileau P (2000). “Latarjet-Bristow procedure for recurrent anterior instability”. Tech Shoulder Elbow Surg. 1: 256–61.