
Case 7: Ultrasound and early detection of Stress Fracture in a runner
Stress injuries are a common cause of lower limb pain in runners accounting for approximately 8% of all injuries in elite track and field athletes (1). Bone stress injuries often progress to stress fractures (2). Stress fractures are the result of accelerated physiologic change from excessive loading applied to a normal bone (3) following a combination of high intensity, duration of training, nutrition, biomechanical and hormonal imbalances (2). Typically in runners it is the 2nd and 3rd metatarsals and the lower tibia which are affected.
The sensitivity of standard radiography which may miss a stress fracture in the early stages due to an absence of callus formation can be as low as 10% (4). Although MRI provides excellent sensitivity it is associated with relatively high cost and accessibility.
Although MRI may be considered the gold-standard for the evaluation of stress fracture, ultrasound is able to pick up early and subtle changes. Both cortical irregularities and hypertrophic changes may be seen before they are visualised on plain XR. Sensitivity and specificity of ultrasound compared to MRI is inferior (sensitivity 82%, specificity 67%). However given the increasing accessibility of ultrasound, the speed and cost of an ultrasound scan it is well worth considering as an alternative imaging modality.
The characteristic features of a stress fracture seen with ultrasound are,
- Hyper or hypoechogenicity of the adjacent soft tissue indicating soft tissue oedema and inflammatory change.
- Thickening of the periosteum.
- Cortical disruption.
- Increased Doppler flow within the periosteum.
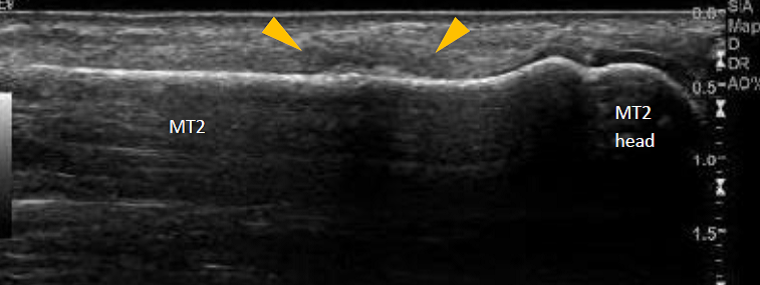
The case below is of a 40 year old female runner with pain in the midfoot. She could describe no initiating trauma or any significant change in her training workload. Plain XR’s were unremarkable at 3 weeks following onset of symptoms.

Plain XR demonstrated no evidence of stress fracture in this runner
An Ultrasound demonstrated evidence of cortical disruption and periosteal oedema seen as hypoechoic swelling in keeping with a stress fracture. The Ultrasound took 2 minutes to complete and saved referral for MRI.
- Papalada A, Malliaropoulos N, Tsitas K, et al (2012). Ultrasound as a primary evaluation tool of bone stress injuries in elite track and field athletes. Am J Sports Med. 40: 915-919.
- Reeder M T, Dick B H, Atkins J K, Pribis A B, Martinez J M (1996). Stress fractures: current concepts of diagnosis and treatment. Sports Med. 22: 198-212.
- Geslien G E, Thrall J H, Espinosa J L, et al (1976). Early detection of stress fractures using 99mTC-polyphosphonate. Radiol. 121: 683-687.
- Greaney R B, Gerber F H, Laughlin R L, et al (1983). Distribution and natural history of stress fractures in US Marine recruits. Radiology. 146: 339-346.