Boxer’s Knuckle
Direct trauma to the dorsal aspect of the MCP joint of the fingers is a common occurrence in Boxers and Martial Artists. This injury to the extensor mechanism has been called a “Boxer’s knuckle” although this should not be confused with the term ‘Boxer’s knuckle’ used to describe a fracture of the 5th metacarpal. The fracture of the 5th metacarpal is more likely to be due to a ‘pub fight’ as a Boxer would not hit you with his little finger!
Functional Anatomy
The anatomy and the function of the extensor mechanism is complex and consist of a linkage system created by the radial nerve innervated extrinsic system and the ulnar and median nerve innervated intrinsic system. The extrinsic extensors to the fingers arise in the forearm and comprise of extensor digitorum, extensor indicis and extensor digiti minimi.
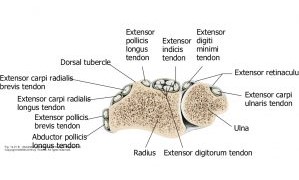
They enter the hand through six compartments formed by the extensor retinaculum. The first longus and brevis, the third extensor pollicis longus, the fourth extensor digitorum and extensor indicis, the fifth extensor digiti minimi and the sixth and most medial extensor carpi ulnaris. At the wrist the tendons are covered by a synovial sheath but not over the dorsal hand or fingers.
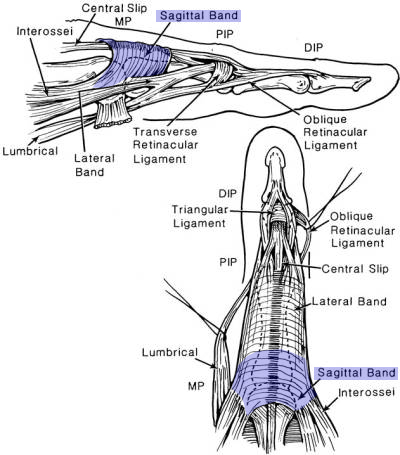
As the extensor tendons approaches the metacarpophalangeal joint, they spread out to form the dorsal digital or extensor expansion, also described as the extensor hood. This is a fibrous expansion over the dorsum of the proximal phalanx of each digit. It can be regarded as an aponeurotic extension of the tendon of extensor digitorum.
Each expansion forms a moveable hood which moves distally when the metacarpophalgeal joint is flexed and proximally when it is extended, in which position it is most closely applied to the joint.
The expansion is triangular, and the base of the triangle, which is proximal, wraps around the dorsal and collateral aspects of the metacarpophalangeal joint. A tendon of extensor digitorum blends with the expansion along its central axis, and is separated from the metacarpophalangeal joint by a small bursa. The base of the expansion, which connects this tendon to the adjoining interosseous muscles on each side, is stabilized by numerous transverse fibres and by links that extend to the deep transverse metacarpal ligaments.
As the tendon of extensor digitorum approaches the proximal interphalangeal joint, it divides into a middle and two lateral slips. The middle slip passes across the joint and carries the main insertion of the extensor into the base of the middle phalanx. The two lateral slips converge over the middle phalanx, and unite to be inserted into the base of the terminal phalanx. The lateral slips are joined by parts of the tendons of the interossei and, on the radial side, by the tendon of the lumbrical muscle. Thus both the interossei and lumbricals are inserted into the base of the terminal phalanx via the lateral slips.
At the MCP joint the extensor mechanism is comprised of the longitudinal extensor digitorum tendon and the transverse peripheral fibers, termed the sagittal bands. Intact sagittal bands prevent subluxation of the extensor digitorum tendon. The extensor tendons are also stabilized by the juncturae tendinum, which are fibrous connections between the tendons proximal to the MCP joints. Beneath the extensor expansion is the thick dorsal capsule, which contributes to protection of the MCP joint. These structures are maximally stretched over the metacarpal head as a fist is made, making them more susceptible to injury. The index and small fingers each have two extensor tendons crossing the MCP joint each lying on the ulnar side of the common extensor tendon. The index finger has the extensor indicis which shares the same synovial sheath as extensor digitorum in the 4th dorsal compartment. The small finger has the extensor digiti minimi whose tendon, after passing through the 5th dorsal compartment, splits into two parts. The medial part takes the main share in forming the expansion on the first phalanx. The lateral part, before it joins the expansion, is joined by the tendon from the extensor digitorum.
Pathology
Traumatic soft tissue injuries to the metacarpophalangeal (MCP) joint may result from repetitive or isolated forceful blows with the clenched fist. The most commonly described injury is disruption of the sagittal band of the extensor tendon mechanism. This may be isolated or combined with a more serious and disabling extensor expansion disruption with dorsal capsular rupture.
The term “Boxer’s knuckle” was first coined by Gladden (1957) who used the term to describe four types of injury each representing an increasing degree of pathology to the dorsal region of the metacarpophalangeal joint. In all instances there was swelling about the affected knuckle and thickening of the soft tissue,
- Type I. Thickening of the soft tissue, including the tendon and capsule over the distal end of the metacarpal bone, with no evidence of a tear.
- Type II. Thickening of soft tissue, tendon and capsule over the affected joint, with tear of the more superficial portion of the soft tissue.
- Type III. Thickening of soft tissue, tendon and capsule, over the affected joint, with tear of soft tissue and tendon.
- Type IV. Thickening of soft tissue, tendon and capsule, with tear of these structures, the defect extending into the joint space.
In this case the patient was a 32 year old male semi-professional Boxer. He described a sudden acute pain over the MCP joint of the right middle finger during a training session on a heavy punch bag approximately 2 months previously. He described not having used any supportive wraps.
He had self-medicated with Ibuprofen and described symptoms as having settled although he had been unable to return to any training that involved direct contact against the knuckle.
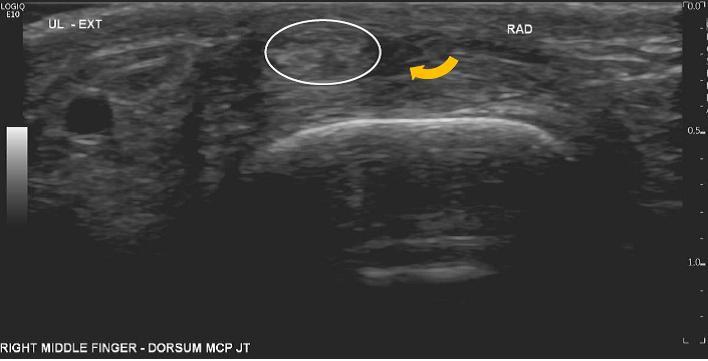
Clinically in flexion the MCP joint of the middle finger appeared ‘flat’ in flexion and with active movement there appeared to be a subluxation of the extensor tendon towards the ulnar side of the joint. This reduced in extension of the MCP joint.
In the ultrasound images below the extensor tendon maybe seen as the white oval. In extension the tendon is seen to lay over the metacarpal head although a little to the ulnar aspect. In addition there is a hyopechoic region to the radial side of the tendon (yellow arrow) corresponding to a tear of the radial sagittal band. In flexion the tendon maybe seen to sublux to the ulnar side of the metacarpal joint.