Case 15; The Wrist Joint – Injection
Anatomical Considerations
The radiocarpal joint is an ellipsoid joint formed by the radius and the articular disc proximally and the proximal row of carpal bones distally. The carpal bones on the ulnar side only make intermittent contact with the proximal side — the triquetrum only makes contact during ulnar abduction.
The parts forming the radiocarpal joint (green line – below) are the lower end of the radius and under surface of the articular disk proximally and the scaphoid, lunate and triquetral bones distally. The articular surface of the radius and the under surface of the articular disk form together a transversely elliptical concave surface, the receiving cavity. The superior articular surfaces of the scaphoid, lunate, and triquetrum form a smooth convex surface, the condyle, which is received into the concavity.
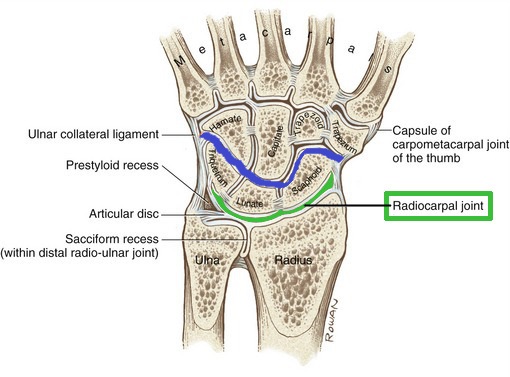 The midcarpal joint (blue line – above) is the S-shaped joint space separating the proximal and distal rows of carpal bones. Although the wrist joint as a whole is not continuous having various internal septa dividing it into separate compartments a variable degree of communication exists with the radiocarpal, intercarpal, midcarpal, and carpometacarpal joints often intercommunicating through a common synovial cavity.
The midcarpal joint (blue line – above) is the S-shaped joint space separating the proximal and distal rows of carpal bones. Although the wrist joint as a whole is not continuous having various internal septa dividing it into separate compartments a variable degree of communication exists with the radiocarpal, intercarpal, midcarpal, and carpometacarpal joints often intercommunicating through a common synovial cavity.
This intercommunication can work to the advantage of the patient with generalised arthritic change as one injection into the radiocarpal and another into the midcarpal joint is likely to perfuse throughout the wrist.
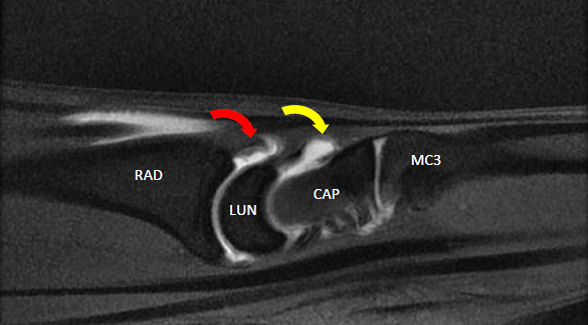
MRI (T1 fat sat) – This sagittal view demonstrates some fluid in the dorsal recesses of both the radiocarpal joint (read arrow) and midcarpal joint (yellow arrow).
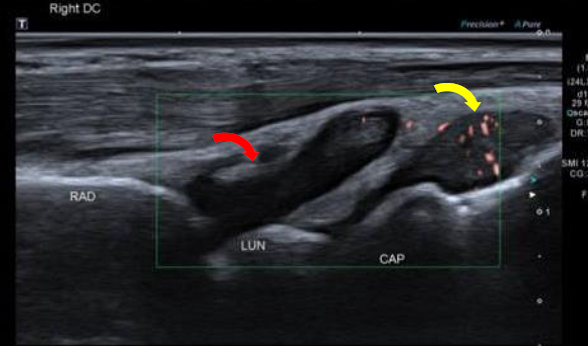
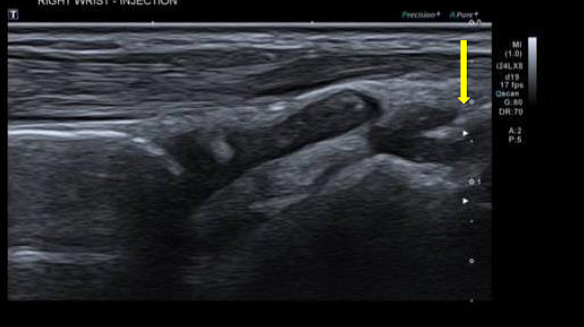
The US view below is in the same plane and same patient as the MRI above although demonstrates a significantly larger effusion at the radiocarpal joint (red arrow) than MRI.
Injection Technique
- The patient is seated facing the clinician with the forearm and hand resting on a table palm facing down.
- The transducer is placed in the longitudinal plane over the mid-point of the dorsal aspect of the wrist joint. In this position it should be possible to visualise the distal radius, lunate and capitate.
- The needle is inserted at approximately 45 degrees to the transducer from a distal to proximal direction. The needle should lie along and parallel to the posterior surface of the lunate.
- The injection maybe given as a bolus into the radiocarpal and then the midcarpal joint if required.

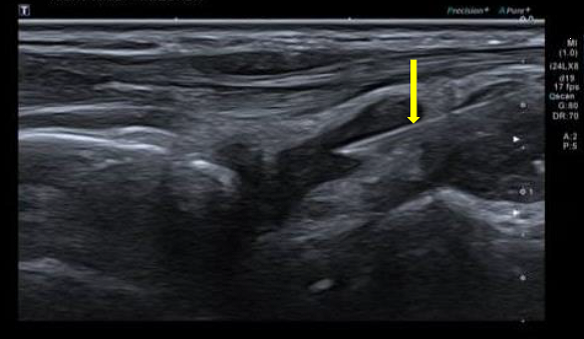
In the image below the the needle maybe seen entering the midcarpal joint capsule (yellow arrow).
Following injection into the midcarpal joint the needle was re-positioned (it does not need to be completely removed) into the radiocarpal joint – below.